Safety
How safe is it?
Recent Anesthesiology Literature estimated the risk of Anesthesia performed by a Dentist Anesthesiologist for dental procedures is 1in 2,000,000 to 1in 4,000,000. Having a Dentist Anesthesiologist to administer the Sedation/General Anesthesia allows the treating Dentist to focus solely on the dental procedures.
Any Dentist Anesthesiologist holding a current General Anesthesia Permit from the California State or Nevada State Dental Boards is well trained and qualified to administer a safe anesthetic for your dental procedures.
Be sure to check that your Dentist Anesthesiologist has a current General Anesthesia Permit and has current B. L. S., A. C. L. S. or P. A. L. S. certificates.
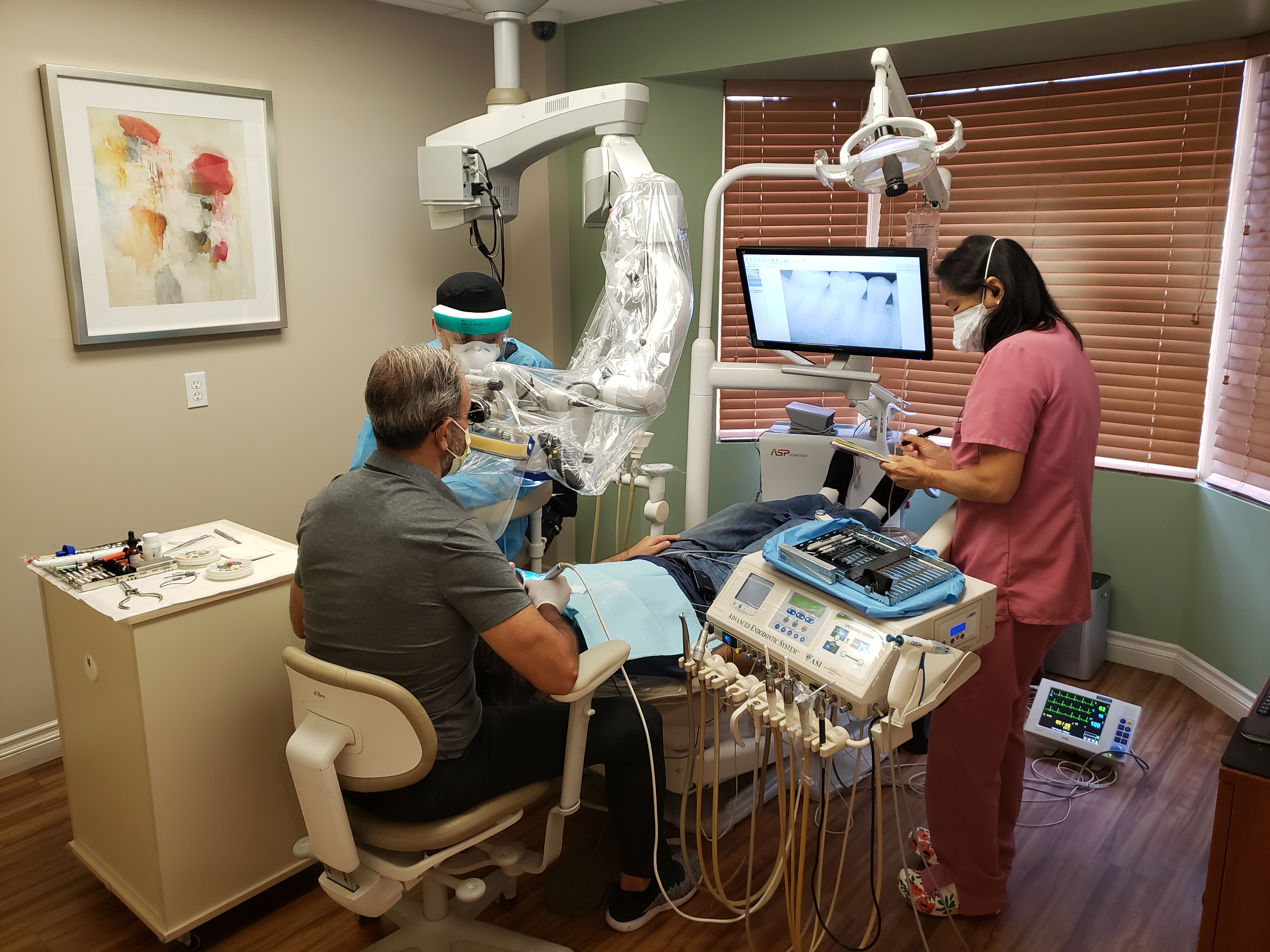
By State Law, each procedure will have the equipment equivalent to that in an ambulance in the dental office, at chairside and ready for each sedation. This includes emergency medications and equipment for any possible complication.
Continuous oxygen is administered throughout treatment and into recovery.
You or your child are safer under sedation with a Dentist Anesthesiologist than in a car on the road
Monitors used
Pulse Oxymetry is a continuous and noninvasive way to monitor saturation of Oxygen bound to arterial Hgb (Oxyhemoglobin) cells in the periphery. This reliable monitor is an early warning sign of Hypoxemia (Decrease of Oxygen in the blood). The Pulse Oximeter is a finger clip that transmits light through the finger and calculates the % of light that gets absorbed by the Oxyhemoglobin versus the De-Oxygenated Hemoglobin. Nail polish may alter the accuracy of the calculation of Pulse Oxymeter. The Pulse Oxymeter values are recorded throughout the procedure and into recovery until the values are stable when the supplemental oxygen is removed.
Blood Pressure is monitored with a Non-Invasive Cuff placed on the upper arm or lower leg. The Anesthesia monitor is set to automatically check the Blood Pressure every 2 ½ minutes, for children, and every 5 minutes, for adults. Blood Pressure is recorded and documented throughout the procedure and recovery.
Pre-Cordial Stethoscope is a weighted Stethoscope placed at the base of the neck and connected to the Anesthesiologist’s earpiece. This stethoscope is used to hear every heartbeat and every breath. The stability, consistency and quality of each heartbeat and respiration are monitored.
Electrocardiography (E. K. G. / E. C. G. ) is a continuous display of the electrical activity of each heartbeat. This is used to determine the Heart Rate and detect irregular heart rhythms and myocardial ischemia (the first signs of a Heart Attack). The Heart Rate and Rhythm is documented throughout the procedure and recovery.
Respiration Rate is calculated by the E. K. G. / E. C. G. monitor. And confirmed by the Precordial Stethoscope.
Patient inidividuality
Every person is different and it is impossible to accurately predict an individual patient’s specific response to any medication. About 80% of people respond within a predictable range (the Bell Curve), but the rest can be considered either super/hyper-sensitive or resistant/hyposensitive to the medication. It is virtually impossible to determine your reaction to a particular medication without past experiences. A convenient example of this type of variance is found in drinking alcohol. Some people need 5 drinks to achieve the similar effects of another person needing only 1 or 2 drinks. One set dose may not be adequate for a resistant person and toxic to a hypersensitive person. Thus, the Intravenous route provides superior control of the effects of any medications and with small incremental dosing, may be precisely tailored to the individual patient and their responses.
Medications taken Orally are effected by the “First Pass Phenomena.” When a medication is taken orally, it first must survive the acidic environment of the stomach and bile. The % of molecules that remain intact is unpredictable and dependent on the specific chemistry of the stomach at that particular moment. The intact active molecules will then be absorbed by the venous system of the stomach lining and transported directly to the liver. The liver then metabolizes a large % of the molecules before the remaining intact active medication has a chance to reach the general circulation and C. N. S. to become effective. The duration and depth of the medication’s effects is also unpredictable since it is dependent on the activity of the stomach and the liver. It is difficult if not impossible to adjust the duration or level of sedation safely.
The advantage of having medications delivered by I. V. Sedation/General Anesthesia by a trained Dentist Anesthesiologist, is that the medications are individualized to the specific needs of the patient. The specific medications that I use are selected for their safety, immediate action, accuracy and predictability. The medications will be administered slowly and cautiously without any set dosing to allow the anesthesia to be specific to the needs of each individual patient. A great advantage is that there is no memory of the procedure. Multiple procedures and multiple appointments can be completed in one session without the risk of emotional trauma. Newly developed medications tailored for the needs of dental procedures make I. V. Sedation/General Anesthesia safer than ever before. With an experienced Anesthesiologist dedicated solely to the anesthesia, the Dentist is free to concentrate on the dental procedures. Efficiency and precision are maximized.
Common medications
Benzodiazepins:
- Has a reversal agent (Flumazinil)
- Sedative and calming effects
- Metabolized by the Liver
- Relative safety if taken in overdose
Midazolam/versed
- Rapid onset (30-60 seconds)
- Short Acting
- Amnesia
- Minimal depression of the Respiratory System (Breathing Rate and Volume)
- Minimal depression of the Cardiovascular System (Heart Rate and Blood Pressure)
- Rarity of Physical Dependence
- Rapid Elimination (1-4 hrs) which aids in a more rapid recovery
Diazepam/Valium (I. V. & oral)
- Painful on injection (inject slowly into large vein)
- Long acting secondary to Active Metabolites with elimination at 21-70 hrs
- Insignificant Amnesia
- Some Respiritory and Cardiovascular Depression
- Return of Drowsiness may occur 6-8 hrs after initial dose because of Recirculation of Active Metabolites. This may occur at home without healthcare providers present. Longest recover of the Benzodizepines.
- Often used for seizure control
Lorazepam / Ativan(oral)
- Peak effect 2 hrs after oral administration
- Long acting with elimination at 10-20 hrs
- Moderate Amnesia
- Unpredictable Blood Level- C. N. S. Response Relationship
- Unexpected Cardiovascular and Respiratory Depression when combined with Opioids
- Caution with patients over 65 yrs
- Not recommended for children under 12yrs
- Longer recovery compared with Versed
Triazolam/halcion (oral)
- The F. D. A. does not recognize use for Dental or Pediatric Sedation. F. D. A. Approved as a Sleep Aid
- The Upjohn Company, which distributes Halcion makes no claims of its usefulness as a Dental Sedative and is not supported or encouraged by the company.
- Should not be used on any patient in a non-hospital/surgical center setting who has any medical condition(s) however slight.
- Peak effect 1-1.5 hours after initial dose (more rapid if taken sublingual (dissolved under the tongue))
- Amnesia
- Undetermined Active Metabolites causing prolonged effects
- Elimination ½ life 1.5-5 hrs. May be prolonged with Erythromycin, Tagamet, Oral Contraceptives, and Isonazid (used for Tuberculosis).
- Minimal effects on Cardiovascular and Respiratory Systems Blood Pressure and respiration monitors required.
- Considered oversedation if patient sleeps during procedure. Verbal contact should be maintained
Opioids:
- Has reversal agent (Naloxone)
- Euphoria & Analgesia (Pain Relief)
- Mild to Moderate depressive effects on Cardiovascular and Respiratory Systems
- Metabolized by the Liver
Morphine sulfate / Morphine
- Releases Histamine
- Causes some Nausea/Vomiting
- Duration 2-7 hrs
- Causes Constipation
Fentanyl / Sublimaze
- Rapid onset
- Short duration 30-60 mins
- Cardiovascular Stability
- Repeated doses have the potential for cumulative effects including Respiratory Depression
- 75-125 times more potent than Morphine
Alfetanil/Alfenta
- Most rapid onset
- Most rapid elimination
- Moderate Cardiovascular and Respiratory Depression
- Repeated doses do no result in accumulation; rapid recovery and minimal post-operative respiratory depression
- 25 times more potent than Morphine
Sufentanil/Sufenta
- Prominent slowing of the Heart Rate
- Short duration 20-45 mins
- Moderate cardiovascular and Respiratory Depression
- 500-1000 times more potent than Morphine
- Repeated doses have the potential for cumulative effects including Respiratory Depression
Ketamine:
- Dissociative Anesthetic
- Rapid Onset 1-2 minutes
- Rapid Elimination 16-18 minutes
- Cardiac and Respiratory Stimulation
- Hypersalivation
- Amnesia
- Eyes remain open with eyes darting from side to side
- Intense Analgesia
- Increased skeletal Muscle Tone which helps maintain the airway
- Hypo-Allergenic
- Concurrent use of Benzodiazepines may reduce the incidence of Emergence Reactions
- Metabolized by the Liver
Propofol/Diprivan:
- General Anesthesia and Sedation
- Rapid onset 30-90 Seconds
- Elimination 30-60 minutes
- Rapid awakening. Awakening is more rapid and complete than with any other I. V. anesthetic
- Mild and Dose dependent depression of Cardiovascular and Respiratory Systems
- Repeated dosing has Minimal Cumulative Effects
- Painful on injection large vein preferred
- Decreased incidence of Nausea/Vomiting
- Metabolized by the Liver
References:
- Stoelting, R. K., Miller, R. D., Basics of Anesthesia 3rd Edition, 1994 pages 62-71.
- Omoigui, S., The Anesthesia Drugs Handbook 2nd Edition, 1995 pages 4-338.
- Various Handouts from Dental Anesthesia conferences.
latest news
- Really under During Surgery? Monitor Can Tell (opens in new window)
- American Dental Association News (opens in new window)
- American Academy of Pediatric Dentistry (opens in new window)
- Anesthesia Safety (opens in new window)
- Levels of Sedation (opens in new window)
- Sedation and Dentistry (opens in new window)
- I V sedation vs Oral sedation (opens in new window)
- More links >>>
Information and Links
Partners